68%
of hospital AI implementations report no measurable workflow improvement after 12 months
ISO 13485: 2016 Certified - Software as a Medical Device (SaMD)

Every AI sold to hospitals today is a tool—something you pick up, use, and put down. What if it was the environment your clinicians lived and worked inside every single day?
Ayesha Khan · June 2026 · Max 10 min read

Every hospital procurement team has sat through the same presentation. A new AI vendor. A new benchmark. A higher AUC score on a new dataset. A promise that this time, the workflow will change. It rarely does.
The problem is not the model. The problem is that every AI being sold to hospitals today is a tool, something you pick up, use, and put down. A second opinion engine. A flagging system. A detector sitting at the edge of a workflow that was built in 2009 and has not moved since.
What if the AI was not a tool you reached for, but the environment your clinicians lived and worked inside every single day?
That is the shift PRAID AI was built around. Not a better detector. Not a higher score on a curated dataset. A clinical environment, one where radiology and pathology work side by side, where every interaction trains the system, and where the infrastructure you already own gets smarter without being replaced.
68%
of hospital AI implementations report no measurable workflow improvement after 12 months
4.2×
average number of disconnected AI tools in a mid-size hospital radiology department
$2.8M
average annual cost of radiologist burnout-related turnover per 100-bed hospital
Sources: KLAS Research 2024 · Definitive Healthcare · Journal of the American College of Radiology
Hospitals have spent the last five years buying AI by the piece. A nodule detector here. A fracture flagging system there. A separate pathology solution from a different vendor with a different login and a different dashboard.
The result is a fragmented stack, multiple systems that do not talk to each other, requiring clinicians to switch contexts dozens of times a day, feeding data into silos rather than a shared clinical intelligence layer. This is not an AI problem. It is an architecture problem. No amount of accuracy improvement on any single model will solve it.
| Capability | Traditional AI Tool | OEM-Embedded AI | PRAID AI |
|---|---|---|---|
| Works on existing PACS/LIS/RIS | Often requires migration | Locked to hardware | ✓ Vendor-neutral overlay |
| Radiology + Pathology unified | Siloed by modality | Hardware-specific | ✓ Single environment |
| Learns from institutional data | Static post-deployment | Vendor-controlled | ✓ Continuous flywheel |
| Built-in teaching & training | External/separate | Not included | ✓ Native learning portal |
| Voice + annotation + co-pilot | Add-on integrations | Limited to modality | ✓ Native in one loop |
| No rip-and-replace required | Varies | Requires vendor HW | ✓ Overlays existing infra |
PRAID AI was designed around a single principle: the most powerful AI is the one your clinicians actually use, consistently, every single day. That only happens when the AI becomes the habitat, not a detour.
Radiology and pathology sit side by side in this environment, not in separate platforms, not with separate logins, not requiring a bridge integration. When a radiologist flags a finding and a pathologist correlates it, both perspectives are captured and fed back into the same intelligence layer.
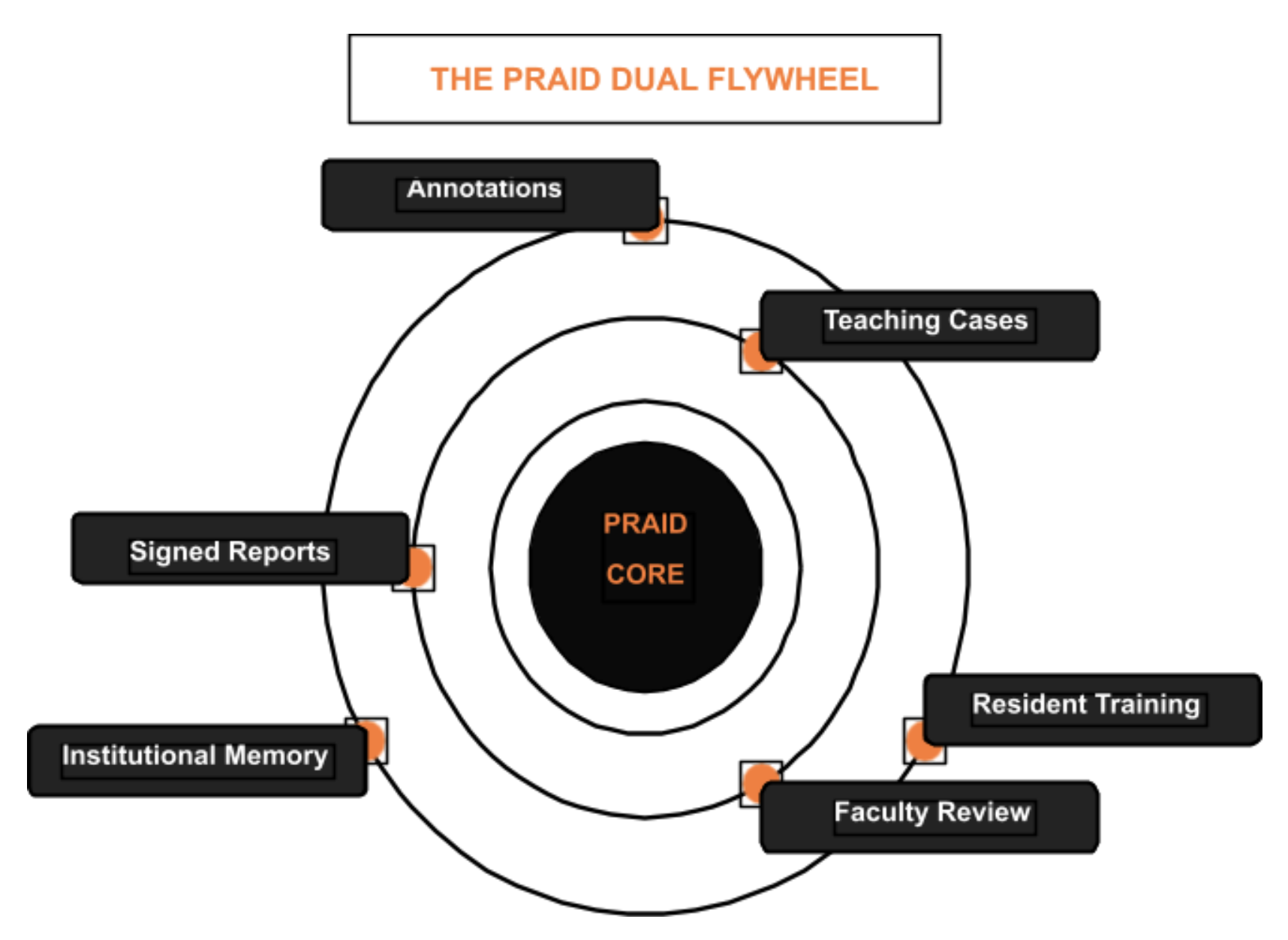
Every signed report becomes training data. Every annotation becomes a teaching case. The radiology and pathology learning portals are not add-on features, they are what the system naturally produces while it runs. Residents learn from real institutional cases. Faculty review at scale. Quality improves continuously, not in update cycles.
A tool improves when the vendor ships an update. An environment improves every single day your clinicians use it.
The market rewards a better product for a quarter. It rewards the better habit for a decade. Consider what actually drives long-term clinical AI value in a hospital setting:
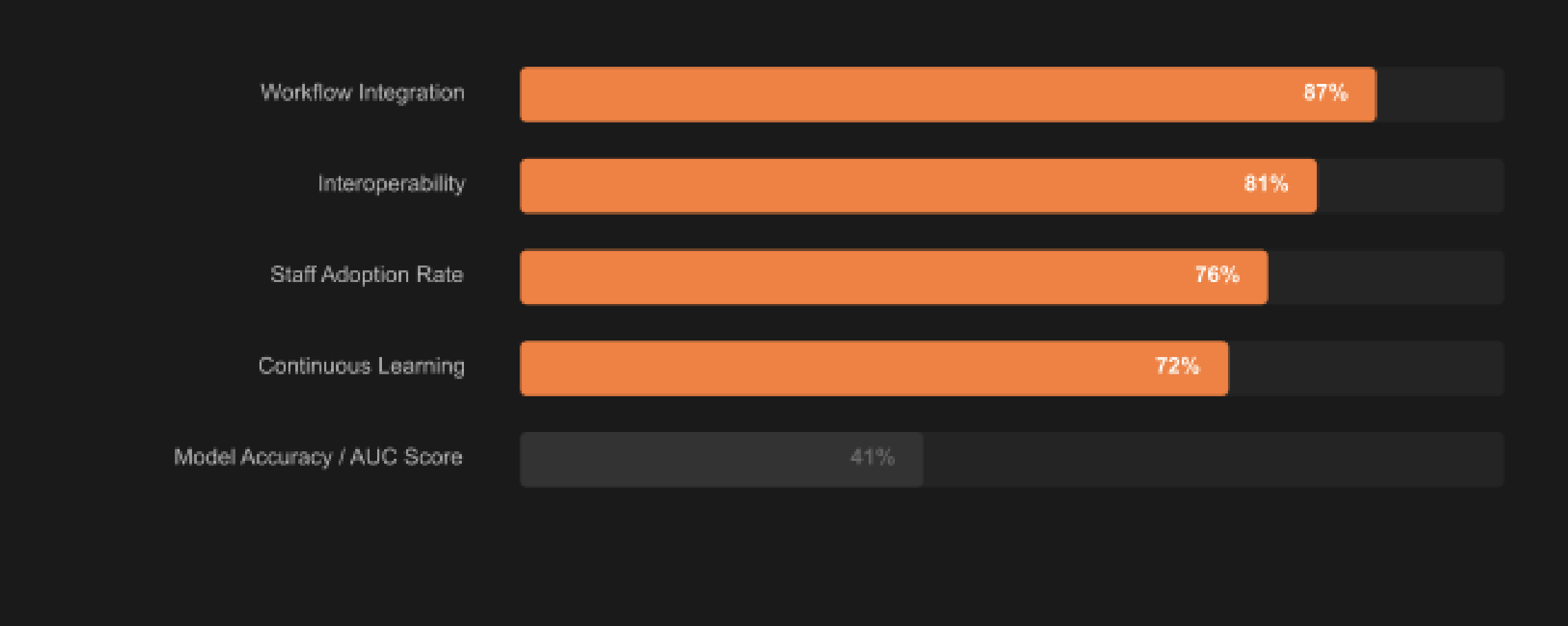
Source: KLAS Research - AI in Clinical Imaging 2024 Report

PRAID is not competing on AUC. It is not entering the race for the highest segmentation score on the latest pathology dataset. That race is real, but it is not the race that changes how a hospital operates, how a resident learns, or how a radiologist experiences their day.
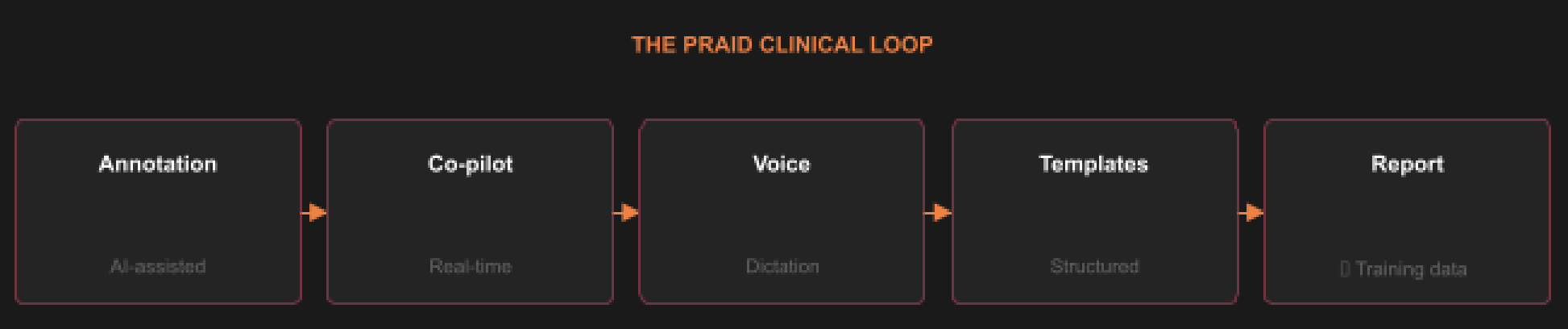
PRAID AI is a vendor-neutral clinical overlay that sits on top of your existing PACS, LIS, HIS, and RIS infrastructure. No rip-and-replace. No migration. No new hardware dependency. It connects radiology and pathology in a single environment, closes the reporting loop with voice, annotation, co-pilot, and templates, and turns every interaction into institutional intelligence.
Accuracy is a feature. The environment is the product. And the environment compounds every single day it is in use.
Built for GCC. Built for KSA. Built for North America and Europe. Built for the hospital that is tired of buying tools and ready to build a habit. Built Global.